
Translate this page into:
Myocardial infarction in non-obstructive coronary artery (MINOCA) in a young girl with multidrug poisoning
* Corresponding author: Md. Moniruzzaman, Department of Cardiology, Sheikh Fazilatunnessa Mujib Memorial KPJ Specialized Hospital, Gazipur, Dhaka, Bangladesh. dr.zaman41@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Moniruzzaman M, Paul AK, Bulbul KMA, Islam MS, Hasan MN. Myocardial infarction in non-obstructive coronary artery (MINOCA) in a young girl with multidrug poisoning. South Asian J Health Sci. 2024;1:117–9. doi: 10.25259/SAJHS_3_2024
Abstract
A 24-year-old girl was admitted to the emergency room with chest pain, abdominal discomfort and excessive sleeping tendency after taking some unprescribed medications. She had no risk factors for cardiovascular disease. On query, she gives a history of taking multiple medications available in her room due to some emotional outbreak. Her relatives give a history of taking paracetamol 1000 mg, cephradine 2500 mg, propranolol 100 mg, bilastine 160 mg and hydroxyzine 200 mg. None of these drugs have proven to cause myocardial infarction (MI) at this dosage. Initial ECG showed sinus bradycardia which can be because of taking propranolol. But 2 hours after admission, she developed severe chest pain and at that time ECG showed gross segment (ST) depression. Troponin-i was found to be raised. After initial management, a coronary angiogram was done which revealed normal epicardial coronaries. Patient was managed symptomatically and she recovered completely.
Keywords
MINOCA
Young girl
Multidrug poisoning

INTRODUCTION
MINOCA is defined as evidence of Myocardial Infarction in the absence of obstructive coronary arteries.[1] In MINOCA, despite angiographic evidence revealing normal or nearly normal coronary arteries (stenosis <50%), patients present with clinical signs and symptoms of Myocardial Infarction (MI). Almost 1–14% of MI occurs in the absence of obstructive Coronary Artery Disease (CAD).[2–3] As treatment modalities are different between MI and MINOCA, proper understanding of the pathophysiology is crucial for appropriate evaluation and management. However, there is no previous literature based on randomised control trial suggesting drug toxicity as a direct risk factor that leads to the symptoms [Figure 1]. In this case report, a young lady with no previous illness developed bradycardia followed by significant ST change in ECG along with raised troponin-i level after taking multiple drugs at a non-toxic dose. Coronary angiography was carried out immediately. However, no signs of obstruction were detected. Hence, a suspicion towards drug-induced MINOCA was raised.
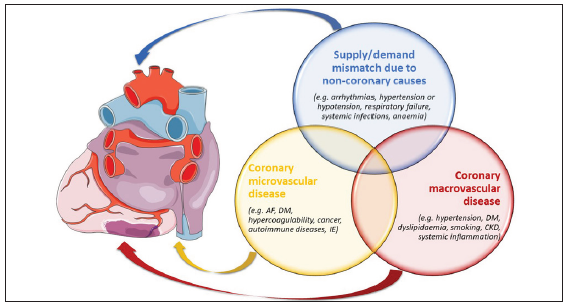
- Risk factors and comorbidities of MINOCA. AF: Atrial Fibrillation, DM: Diabetes Mellitus, IE: Infective Endocarditis, CKD: Chronic Kidney Disease, MINOCA: Myocardial Infarction in Non Obstructive Coronary Artery.
CASE REPORT
A 24-year-old lady presented with complaints of central chest pain, abdominal discomfort and excessive sleeping tendency. Upon further inquiry, she reported ingesting multiple unprescribed medications in response to an emotional outbreak. She did not have any significant past medical illness and denied having any of the chronic medical conditions. She is not an alcoholic and does not smoke. Further probing on psychiatric illness and recreational drug abuse was found to be insignificant. Upon initial examination, the patient appeared distressed and exhibited signs of discomfort. Vital signs revealed sinus bradycardia on a cardiac monitor, which was attributed to the ingestion of propranolol. However, 2 hours after admission, she developed severe chest pain, which was similar to cardiac-type chest pain.
Patient’s initial ECG showed sinus bradycardia [Figure 2a], likely secondary to propranolol ingestion. However, the subsequent ECG after 2 hours exhibited gross ST-T changes in most leads, correlating with the onset of severe chest pain [Figure 2b]. Laboratory investigations revealed elevated levels of Troponin-i- 44.6 ng/mL, indicating myocardial damage. Routine blood investigations reveal nothing significant. A quick echocardiography was arranged, but no structural or functional abnormality was evident. A coronary angiogram was performed to assess coronary artery patency, which surprisingly revealed normal epicardial coronaries, ruling out traditional ischemic aetiologies [Figure 3].
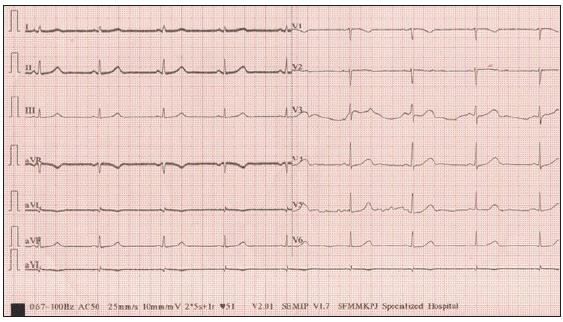
- ECG during initial assessment showing sinus bradycardia.
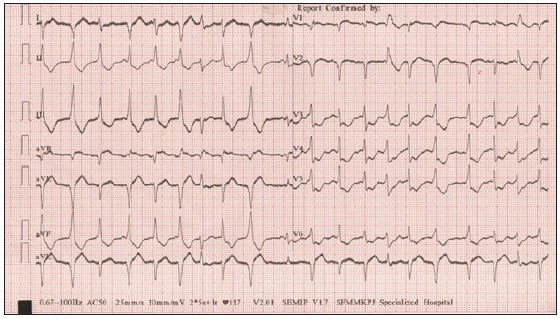
- ECG after 2 hours showing gross ST-T changes. ST: segment, T: wave changes.
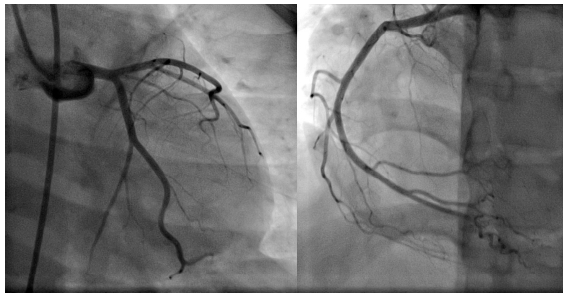
- Coronary angiogram reveals normal epicardial coronaries.
The patient’s symptoms and laboratory findings were consistent with MI despite the absence of traditional risk factors and obstruction in coronary arteries. The aetiology of MI in this case was attributed to the ingestion of multiple unprescribed medications, including paracetamol 1000 mg, cephradine 2500 mg, propranolol 100 mg, bilastine 160 mg and hydroxyzine 200 mg. Although none of these medications are typically associated with MI at these dosages, their combined ingestion likely led to myocardial damage.
The patient was managed symptomatically, with a focus on pain relief, haemodynamic stabilisation and cardiac monitoring. Given the absence of obstructive coronary disease, traditional reperfusion strategies such as thrombolysis or percutaneous coronary intervention were deemed unnecessary. Instead, supportive measures such as fluid management, analgesia, antiemetic, anti-ulcers and close cardiac monitoring were instituted. With time, the patient’s symptoms resolved completely, and she demonstrated clinical improvement. The patient was advised against self-medication and educated on the potential risks associated with unprescribed drug ingestion. Follow-up appointments were scheduled to monitor cardiac function and ensure ongoing adherence to prescribed medications and lifestyle modifications to mitigate cardiovascular risk factors. In addition, psychiatric evaluation and counselling were recommended to address underlying emotional issues contributing to the patient’s self-medication behaviour. Her family members were also counselled.
DISCUSSION
Here we are presenting a young female patient, who has been diagnosed as MINOCA following taking some unprescribed medications that do not cause vasospasm, ulceration and obstruction in the epicardial coronary arteries. Despite having significant ST abnormalities in ECG and raised Troponin-i level, echocardiography and coronary angiographic findings were not suggestive of MI (Invasive provocative coronary vasospasm testing could not be performed due to the acuteness of the situation). Besides, the patient didn’t have any relevant past medical history related to hypercoagulable state and coronary artery disease. Therefore, multidrug poisoning was held responsible for her chest pain, ECG changes and raised troponin level. Moreover, she responded to symptomatic treatment and ECG and troponin level became normal without any intervention.
As per previous study and reports, a few drugs are responsible for MI by causing epicardial vasospasm and toxicity to myocardiocytes. Some chemotherapeutics,[4] antimigraine drugs (triptans),[5] antibiotics (amoxicillin with clavulanic acid, cefuroxime),[6,7] bromocriptine, β-blockers, pseudoephedrine,[8] acetylsalicylic acid (ASA), steroidal and non-steroidal anti-inflammatory drugs[9] are attributed commonly and we know their pathophysiology. But here we did not find any signs of obstruction and signs of toxic myocarditis in CAG and echocardiography, despite having all features of MI in this patient. So, we believe this is a case of MINOCA and a thorough study is needed to find out the drug-related risk factors and their pathophysiological background to facilitate the management approach and avoid irrational invasive procedures.
CONCLUSION
This case report underscores the significance of considering medication-induced MI as a differential diagnosis, especially in young patients with atypical presentations following multidrug abuse. The absence of traditional cardiovascular risk factors and normal coronary arteries on angiogram posed diagnostic challenges, highlighting the importance of a comprehensive evaluation in such cases. Recognising medication-related cardiovascular complications is essential for appropriate management and prevention of adverse outcomes. The management of medication-induced MINOCA requires a multifaceted approach, including symptom relief, haemodynamic stabilisation, psychological support and patient education on the risks of self-medication. Further research is needed to elucidate the underlying mechanisms of medication-induced myocardial injury and to develop targeted interventions to mitigate cardiovascular risks associated with polypharmacy and self-medication.
Ethical approval
The Institutional Review Board has waived the ethical approval for this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Myocardial infarction with non-obstructive coronary arteries: Risk factors and associated comorbidities. Front Cardiovasc Med. 2022;9:895053.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. EurHeart J. 2017;38:143-53.
- [CrossRef] [PubMed] [Google Scholar]
- 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the european society cardiology (ESC) EurHeart J. 2018;39:119-77.
- [Google Scholar]
- 5-fluorouracil-induced cardiotoxicity mimicking myocardial infarction: A case report. BMC Cardiovasc Disord. 2001;1:3.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Triptans and troponin: A case report. Orphanet J Rare Dis. 2009;4:15.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Cefu-roxime-induced coronary artery spasm manifesting as Kounis syndrome. Acta Cardiol. 2005;60:341-5.
- [CrossRef] [PubMed] [Google Scholar]
- Acute ST-segment elevation myocardial infarction complicating amoxycillin-induced anaphylaxis: A case report. Int J Cardiol. 2007;117:e37-e39.
- [CrossRef] [PubMed] [Google Scholar]
- Drug-induced myocardial infarction secondary to coronary artery spasm in teenagers and young adults. J Postgrad Med. 2006;52:51-6.
- [PubMed] [Google Scholar]
- Kounis syndrome secondary to ibuprofen use. Int J Cardiol. 2009;137:e79-e80.
- [CrossRef] [PubMed] [Google Scholar]




